

By Sushmita Solanki
The recent covid 19 Pandemic emphasized the importance of Resilient Health systems, and the crucial role of community health workers within the system, which has been overlooked in pre covid times. The role of CHWs was expanded to meet the needs of the essential healthcare services as well as the pandemic. According to the Decade for workforce strengthening in SEAR 2015- 2024, midterm review the regional average density of the health workforce (doctors, nurses) has improved to 26 per 10,000 population (2018) which is far behind 44 per 10,000, which is required to achieve sustainable development goals. As per Figure 2, India reported 6,989 confirmed COVID 19 cases per 1 million on December 6, 2020 – the largest cumulative number within South East Asia (WHO, epidemiological update). The reported community health workers & Traditional medicine professionals density per 10,000 was 7.2 & 5.9 i.e; 13 in total (WHO, regional office of SEA) which is far below the regional outlier which is 157. In the IHR State Party Self- Assessment Annual Reporting (SPAR) India reported a score of 100% for human resources for the implementation of International Health regulation capacities. The presence of such workforce contributes to the resilience of communities.
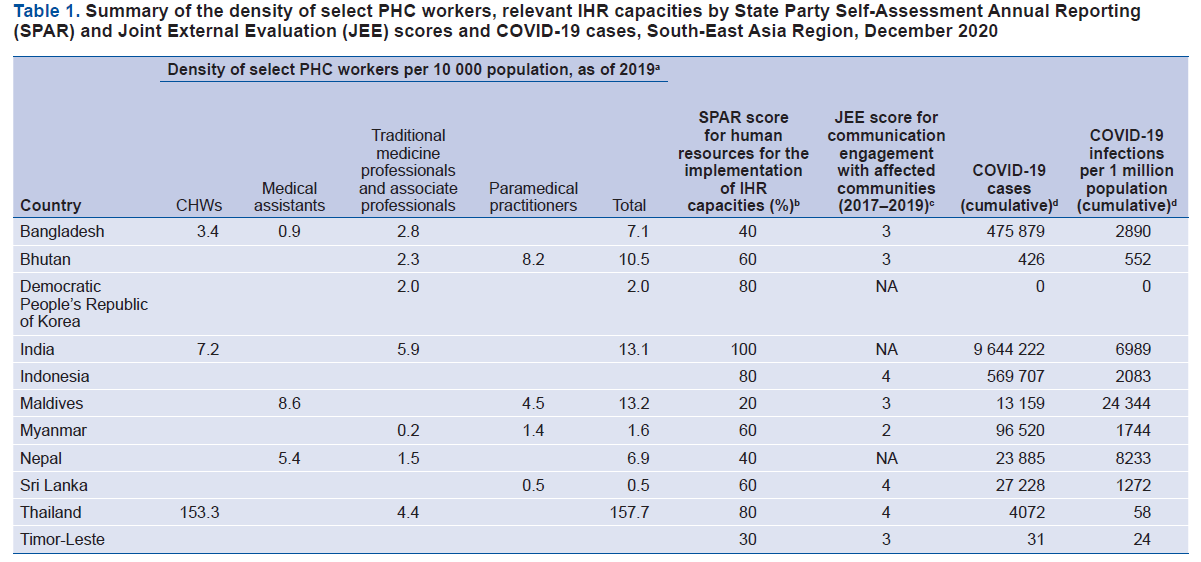
Figure 2
In 2020, the Dharavi model became the talk the nation when this densely populated slum which houses approximately 1 million citizens in just 500 acres, was able to control the transmission chain by adopting the framework called “chasing the virus” with extensive tracing (24 people traced for each case) tracking, testing (13,500 tests) & surveillance. The municipal corporation was able to break the chain through the collaboration of hundreds of CHWs (CORONA WARRIORS). These CHW’s had the community’s trust and were familiar with the space. They performed door to door screening for which they were provided with oximeters, thermal scanners, protective gear (PPE, gloves, shield), and sanitizers. The community kitchen was made functional 24*7 and Dharavi only reported a single case on July 7, 2020 and a total of 2,300 cases due to a strong focus on community engagement.
In Chhattisgarh, frontline workers such as Mitanins (called ASHAs in other states) in the community are a valuable asset in capacity building & preparedness strategies for Covid 19. In March 2020 Covid guidelines were distributed by district & block coordinators to mitanin trainers (each MT has 20 mithanins and covers a population between 7000 to 9000). In rural spaces Handbills were circulated to mitanins which specified the symptoms, behaviours to be followed, & protein intake. Many of them wrote the instructions on the walls. Urban Mitanins ensured food distribution through various state & nonstate actors to 24000 BPL people across 19 urban areas. The food items were stored in the state health resource centre in Kalibadi and an office transport facility was deployed for distribution to different locations. At the same time, they also ensured that the jaundice outbreak was controlled (through tracking & advice). They were aware of the stigma towards people who return from covid facilities and hence they informed people by dispelling misconceptions & rehabilitating the patients in their families & society. In Kathghora, in district Korba, when positive cases were reported, the mitanins escorted the health medical team to collect samples, a buffer area was put up wherein they visited door to door to survey the symptoms such as acute respiratory infection (ARI) were asked to go for testing. The mithanins were provided with masks & hand sanitizers for screening. In Dantewada a COVID19 assistance call centre was established to keep track of individuals that had been quarantined or instructed to isolate at home. The call centre directly connected auxiliary nurse midwives & patwaris for improved coordination. Chattisgarh was able to combat the first wave of covid because of the learnings from past experiences with water-borne jaundice, Japanese encephalitis, Swine flu and dengue.
The key element Kerala capitalised on to fight COVID19 was its strong social agreement between the state & its people, primarily based on the cognizance of the population, paramount social capital (priority to collective good over individual good) & fiduciary relationship with the government. The Kerala government’s learnings from the two successive floods and nipah virus in 2019 made the state manage the shock in a resilient manner. In 2016 the state launched Aardram mission to transform their Primary Health Care and the percentage of people using government facilities jumped to 48% in the 75th round of NSSO. The ASHAs performed 3 tasks to facilitate the Ardram mission- making outpatient tickets and assisting pharmacists and receptionists. Central to Kerala’s public health response were the 28000 ASHA women who were the vanguard of the resistance against the crisis. They diligently collected pre covid data from each household. This complex database recorded women, children 0-5 years, number of people with TB, leprosy, physical disabilities and others which enabled the state to develop a rapid ‘trace-test-isolate-support’ strategy. During the outbreak the ASHAs tracked & traced people with travel history & covid symptoms, reported them to PHCs, escorted them & arranged testing. In January last year a control room had been set up in Thiruvananthapuram to coordinate between 18 rapid response teams at the panchayat level, in which ASHAs were the key participants. Special Covid 19 committees were created at ward level and were fundamentally led by ASHAs due to their previous experience with the Nipah virus. ASHAs worked in community kitchens as well and prepared food for people in containment zones, quarantine, and migrant camps. Overall the ASHAs did all the legwork – from house visits, monitoring quarantine, and collecting data, to coordinating between different departments.
Challenges encountered by CHWs in the COVID-19 response
The ASHAs had received little formal training for carrying out screening of the patients. Majority of the training by the central government was Online which was not accessible to them. They were not provided with sufficient protective gears like gloves, masks, sanitizers to carry out the work. Many frontline workers faced violence on door-to-door visits and were called “CORONA WALLAS”. There was no clarity on what their entitlements were when they were battling a dangerous disease like corona.
A few transcripts from the report interviews conducted by Behanbox which highlight the agony and suffering of the frontline workers in the 16 states.
“A doctor’s job begins only after we have monitored every person in our community and identified people with symptoms,” said Lakshmi. “Yet, when the doctors come into the village they are in full gear, looking like robots, while we are not even given a mask.”
“The PHC staff asked us why we needed masks at all. ‘Are you touching Covid positive patients?’ After a point we had to stop asking because they said we were making excuses for shirking away from our duty,” Pochamma, an ASHA from East Godavari district in Andhra Pradesh said.
“We are called ‘Corona walas’ (Corona carriers) and kept at a distance by our neighbours because we are in touch with community members without proper protective gear”, said Minara Begum, an ASHA from Kamrup district in Assam. “We are paying the price in our community for the government’s inability to keep us safe”, she says.
Present strategy suggested by GOI to combat Covid 2nd wave in rural areas
In May the Ministry of Health & Family Welfare introduced the Standard operating procedure which outlined the containment & clinical management practices to be followed in peri urban, rural & Tribal areas for better third wave covid management & future epidemics/ pandemics.
- Surveillance, screening, isolation, & referral: ASHAs with the help of village health sanitation & nutrition committee (VHSNC) will perform active surveillance on related illnesses periodically. Community health officers & Auxiliary nurse midwives should be trained in performing Rapid antigen tests and these tests should be made available at all the sub centres, health & wellness centres & primary health centres.
- Planning of health infrastructure for managing COVID at rural level: previously a 3-tier structure as put in place. A) covid care centre (CCC) for mild cases, B) Dedicated covid health centre (DCHC) for moderate cases, C) Dedicated covid hospital (DCH) for severe cases. Rural spaces will have a 30-bed facility at CCC and these will be makeshift facilities which will be supervised under the closest PHC. Community health centres/ primary health centres or district hospitals to DCHC. This will also be a minimum 30 bed facility. District hospitals or identified hospitals should be converted into DCHs.
- Human Resource: Anganwadi/ ASHAs will support the ANMs in managing the Covid care centre. VHSC will support the gram panchayats for the upkeep of the facilities. Medical officers of the closest PHC- H&WC will guide the CHWs at the centre. Covid warriors will man the facilities and are deployed at entry/exit point, isolation ward, consultation rooms etc after adequate training of the task.
- Training: Volunteers (selected by VHNSC) will be given elaborate training on performing tests, waste management, infection prevention control.
- Community mobilization & behavioural change communication: A multipronged approach, led by Gram Panchayat and engaging other stakeholders to fight the pandemic.
Key stakeholders within the village community that could be mobilized for COVID-19 management

- Response strategies for tribal areas: Integration of COVID-care with Mobile Medical Units (MMUs) under NHM. The MMUs will provide covid management services and help establish linkage with DHC & DCHC.
Conclusion
CHWs should be included in long term planning & should be recognized as an integral component of the resilient health system. Therefore, planning for, empowering & mobilizing the CHW’s as part of overall health care systems is important such as capacity-building, role clarity, incentives, further training and regulation to ensure preparedness.
Sushmita Solanki is a second-year Masters Student at the Jindal School of Government and Public Policy. Her research interest areas are Urban housing, Health system financing, and Sustainable Development.